Tendinopathy

Written by Paul Norris
(Vertical Junkie, Physiotherapist)
WARNING: LONG AND TECHNICAL READING. May be worth digesting parts at a time and reading referenced research articles as you go along.
Painful elbows suck. Painful fingers suck. Painful Shoulders suck. Now that I have your complete agreement, I could just stop this article there. Unfortunately, I still hear outdated advice almost every time someone mentions their aching elbow in the gym.
Recently I had a chat with Physio and Norweigan Climbing Researcher Dr Gudmund Grønhaug. He touched on an interesting point regarding climbers and their habits of seeking advice (1). It’s all too often that climbers are quick to believe health advice from the crusher in the gym, or the group of peers on the boulder mat, rather than the local health professional.
This leads to a myriad of suggestions, everything from “Brah you have to rest at LEAST 3 months” to “Drink some concrete and get back on your proj” and every weird, quirky treatment protocol in between.
Jokes aside, we won’t delve into why experienced climbers in particular distrust health advice when it comes to climbing injuries, but I will try to clear some things up for the crushers out there!
A good starting point is to address some of the latest concepts in tendon health.
We used to call climbers elbow – epicondylitis. The “itis” component is a suffix which indicates that inflammation is a core part of the issue. Bursitis being inflammation of a bursae, tendonitis being inflammation of a tendon, you get the idea.
So, when you hear someone say elbow tendonitis – they are referring to inflammation as a prime driver of symptoms at their flexor or extensor tendon at the elbow. Inflammation is usually addressed with NSAIDS (ibuprofen etc.), ICE, compression, and rest. Think a swollen ankle in its acute phase.
This issue with this approach is that climber’s elbow pain is commonly elbow tendinosis. We realise this due to the high percentage of climbers who return to sport after rest reporting incomplete recovery and developing chronic problems surrounding injury (3) (4).
TendinOSIS is a DIFFERENT form of tendinopathy (TendinoPATHY is simply an umbrella term for conditions of the tendon, including tendonitis, tenosynovitis and tendinosis).
Notice how we dropped the “itis” suffix. We did this because Tendinosis’ primary issue is not inflammation. For years clinicians have realised this and been referring to tennis and golfers (or climbers) elbow as Epicondylalgia rather than epicondylitis!
WHY IS THIS IMPORTANT?
This misinterpretation is often thought of as simply nit picking on terminology, but this is not the case. Understanding the difference between tendinosis and tendonitis is vital when looking at how to effectively treat and prevent climber’s elbow and other climbing related tendon issues!
SO, WHAT IS TENDINOSIS?
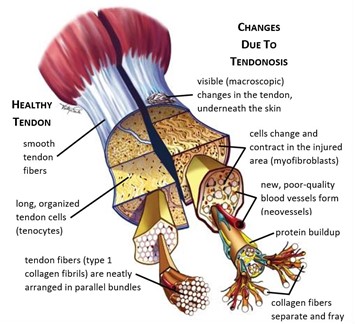
Tendinosis is not local inflammation but is a complete structural and physiological change of the tendon unit. Over time your tendon changes from a neatly structured, highly collagen dense, efficient connective tissue unit to one in disarray (2) (7).
Some of the key changes we see are:
- Fraying and disruption of the collagen fibres. (2)
- Invasion of poor quality neovessels (inefficient blood vessels). (2)
- Increase in mucoid ground substance (extracellular gel type substance) (2)
- Abnormal nerve ingrowth into the tendon unit. (2) (7)
- Changes in the structure of tenocytes (which help synthesise new collagen). (2)
Now let’s be clear. These changes don’t happen from one or two overdone sessions. They are a result of constant overloading and chronic stress on the tendon unit without sufficient recovery over time. (2) (7)

They also can’t be reversed in one or two sessions either! (10) (11) (12)
We all often over do a session, or change a training tool or style which can cause increased load in our connective tissue. With appropriate gradual progression of these new stimulus and with appropriate rest this is usually not an issue and can lead to stronger training adaptations. Some general muscle or joint soreness at this new stimulus can be very normal too.
What is NOT normal is non dissipating, reoccurring pain in the tendon during or shortly after climbing or training. It’s easy to ignore at first, as it doesn’t seem to stop you pulling on, but pay closer attention to your body on this one.
Medical imaging and research indicates that many of the early stages of tendinosis can be ASYMPTOMATIC (13). This means that by the time you have this dull pain, you are likely to already have some of the above structural changes.
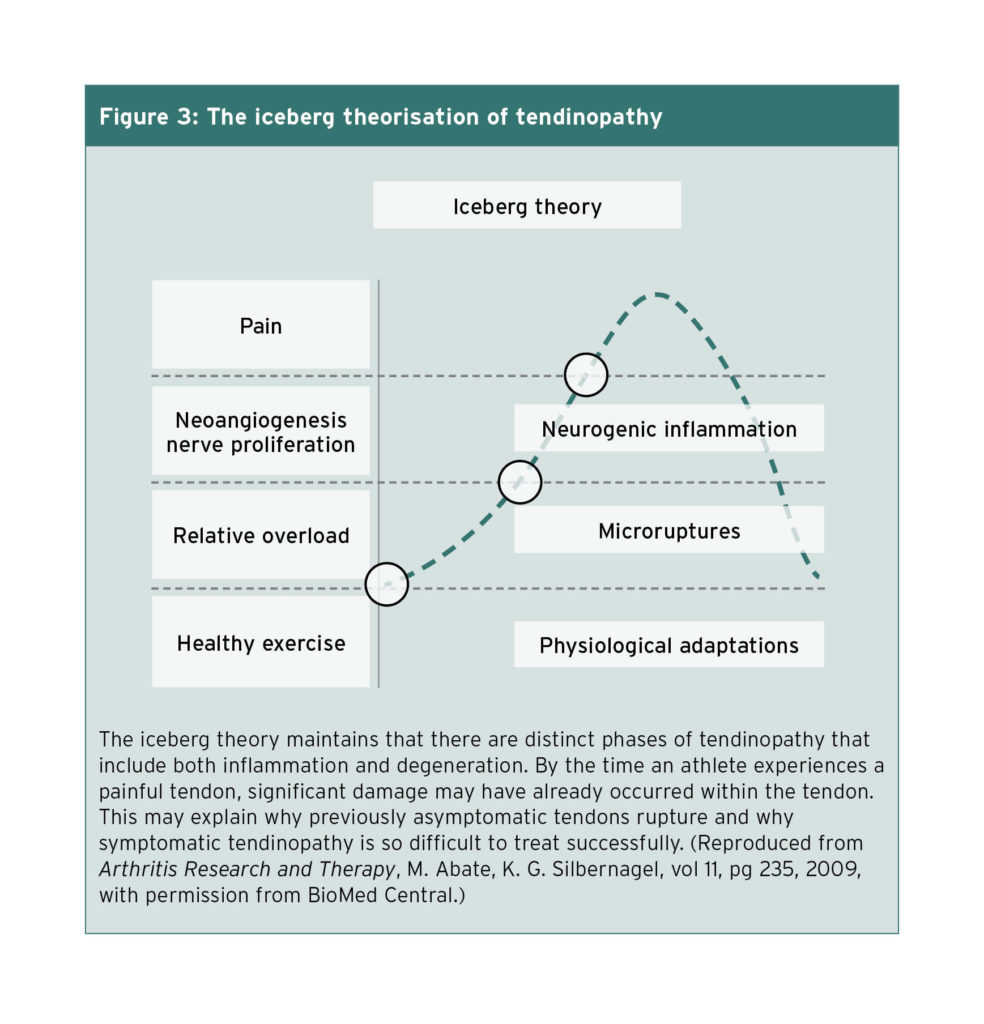
The Iceberg tendinopathy model helps show us that once you have chronic reoccurring pain, it is usually only the “tip of the iceberg”(13).
This dull chronic reoccurring tendon pain is surprisingly poorly understood. One thought is the nerve filaments which have grown into the unstructured tendon by this stage and are reacting to local chemical and mechanical stress. (2) (13) (21) At one point these fibres were thought to be mainly sympathetic (not sensory structures), but recent research has shown that maybe they do play a larger part in reactive and painful tendons.(21)
A good point to keep in mind when programming is that when you load tendons, you get both collagen synthesis AND collagen degradation (14)(15)(16).
This is how the body remodels connective tissue after stimulus to help it adapt and change to meet the demands placed on it.

The body is smart, it doesn’t just lump new collagen on top of the old, but cycles through a process of breaking down collagen to be replaced with stiffer, less stiff, denser, less dense, directional, compression resistant or whatever is required to meet the demands placed upon it. This process takes time, and we can see in the first 36 hours or so following acute exercise, we have a net degradation of collagen (14)(15)(16).
36 hours in we enter a phase where we have a net gain in new collagen, but this collagen is not yet appropriately structured and organised. It is not until 72 hours that the cycle of cleaning up, generation and reorganising of new collagen seems to be nearing completion.
72 hours, that’s three days! I hear you screaming, you can’t keep you out of the gym for three days! And luckily that’s not the end of the story. The degree of reorganisation will likely depend on the stimulus you apply.
All the studies used to create and support this model it seems were based on a very high volume and/or intensity. 1 Hour of continuous kicking at 67% maximal workload (15), 36km run (in conditioned atheletes) (16), etc. I could only find one quality in vitro study (19) touching on the topic – but this requires separate discussion, feel free to read reference 19 for more information.
I would argue you don’t need 3 days rest from a low volume bouldering session climbing perfect repeats. I would also argue limit bouldering followed by a max hang session would benefit from some modulation of tendon load in the upcoming days.
Once again, this ties in heavily to volume management and effective programming which we talk about a LOT at Vertical Junkie.
SO HOW DOES UNDERSTANDING THESE DIFFERENCES AFFECT HOW WE MANAGE TENDINOSIS?
Well, firstly, the over reliance of REST, ICE and NSAIDS is the biggest issue. This is a great strategy for acute tendonitis, or tenosynovitis, but for tendinosis might stunt your journey back to the vertical world.
Now rest is AMAZING – you get stronger from RESTING, not for working out after all. And resting can help to manage pain or a spike in acute symptoms. But long term resting has been shown to be strikingly ineffective for return to sport for tendinosis (11).
Resting does not do anything to change a tendons tolerance to load.
It provides no stimulus to start redirecting healthy collagen synthesis or remodelling. It does not reverse dysfunction. (2)(3)(4)(7)(10)(11)(12)(18)(19)(20).
If you only take one thing from this entire article, take away that statement.
This could explain why climbers rest for months on end, assuming they are “healing” their tendon, and are baffled when symptoms represent almost immediately on return to sport.
It has been shown that the tenocytes which produce collagen not only change negatively due to excessive load, but also respond poorly to a deprivation of mechanical stress (2)(12)(14). Like Goldilocks favourite resting spot, it seems appropriate loads are the sweet spot for these tenocytes, not too hard not too soft!
When it comes to ICE and NSAIDS, they are great sources of pain relief and traditionally used to mitigate local inflammation. Yet you now know that inflammation is not a central or prime driver of climber’s elbow!
For this reason, I caution the implementation of these tools unless necessary for significant pain relief or if diagnosed with a more acute condition as tissue rupture or specifically diagnosed with acute tendonitis / tenosynovitis etc.

WHY WOULD NSAIDS AND ICE SLOW RECOVERY?
To get adaptation in the tendon requires encouraging the tenocytes to respond and adapt to stimulus. For this process to work effectively – the tissue requires increased blood flow and for a multitude of metabolic processes to take place. (I must also mention due to tendons and ligaments having less vascularisation, movement and exercise is important in moving metabolic nutrients into proximity of the damaged tendon!)
Applying ICE and NSAIDS can work to stop or dull these responses, nullifying some of the positive adaptations after you have done your appropriate progressive loading. (6)(9)(14)(17)
Recent research has shown some detrimental effects of NSAIDS and Cryotherapy in strength and endurance adaptations in athletes (9) (and mice!(6)). Interesting reading – we do have to be careful how we extrapolate these studies towards tendon health – so we will keep you updated as more research is published.
What we DO know however, is that an effective loading strategy is KEY to restoring the connective tissue to a healthy state. (2)(7)(10)(11)(12)
This loading will work to desensitise the central and peripheral perception of pain around your tendon, improve net collagen synthesis, reduce neovascularisation and restore a higher percentage of healthy tendon in the tendon unit. (10)(11)(12)(20)
With a catch, and I hate to drop bad news. It seems that severe tendinosis may never return to 100% completely healthy tissue. (2)(7)(20)
The good news? Functionally speaking, this can still allows for a full return to asymptomatic load for the injured climber.
WHAT DOES AN EFFECTIVE, PROGRESSIVE LOADING STRATEGY LOOK LIKE?
Great Question! This article is only the first in a two-part series looking at Tendinosis.
The second section will be available in the Vertical Junkie Members Zone and breaks down what a progressive loading strategy should look like for climbers. We discuss exercise progressions for elbow, shoulder and finger tendinosis, markers for positive adaptations and red flags to be cautious of.
We will touch on some common accessory treatments to these programs too and why they may or may not be a complete waste of your time!
We’ll also deep dive further into programming around Tendon Health and promote some discussions around this topic on the Vertical Junkie Discord.
Look forward to seeing you there!
Written by Paul Norris (Vertical Junkie, Physiotherapist).
Paul is the founder of Vertical Junkie, a climber of 10 years and passionate physio of over 12 years. Paul is one of Alpine IC’s first members, and is a long time friend and training partner. Make sure you check out Vertical Junkie for climbing specific workouts, training programs and injury management, and learn more about how Paul can help you with your climbing goals.
REFERENCES
(1) Grønhaug G. Addressing the elephant in the room: a possible new way to increase patient adherence to
medical advice. Patient Prefer Adherence. 2017;11:1083-1089. Published 2017 Jun 28. doi:10.2147/PPA.S138716, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5499786/
(2) Kaeding C, Best TM. Tendinosis: pathophysiology and nonoperative treatment. Sports Health. 2009;1(4):284-292. doi:10.1177/1941738109337778, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3445129/
(3) Alex K. Folkl,Characterizing the Consequences of Chronic Climbing-Related Injury in Sport Climbers and Boulderers,Wilderness & Environmental Medicine,Volume 24, Issue 2,2013,Pages 153-158,ISSN 1080-6032, https://www.sciencedirect.com/science/article/abs/pii/S1080603212003754
(4) James W. McDonald, A. Michael Henrie, Masaru Teramoto, Edward Medina, Stuart E. Willick,
Descriptive Epidemiology, Medical Evaluation, and Outcomes of Rock Climbing Injuries,Wilderness & Environmental Medicine,Volume 28, Issue 3,2017,Pages 185-196,ISSN 1080-6032,
(5) Huisman E, Lu A, McCormack RG, Scott A. Enhanced collagen type I synthesis by human tenocytes subjected to periodic in vitro mechanical stimulation. BMC Musculoskelet Disord. 2014;15:386. Published 2014 Nov 21.
doi:10.1186/1471-2474-15-386, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4256895/
(6) Machida M, Takemasa T. Ibuprofen administration during endurance training cancels running-distance-dependent adaptations of skeletal muscle in mice. J Physiol Pharmacol. 2010 Oct;61(5):559-63. PMID: 21081799., https://pubmed.ncbi.nlm.nih.gov/21081799/
(7) Mead MP, Gumucio JP, Awan TM, Mendias CL, Sugg KB. Pathogenesis and Management of Tendinopathies in Sports Medicine. Transl Sports Med. 2018;1(1):5-13. doi:10.1002/tsm2.6, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6530902/#R36
(8) Desmeules F, Boudreault J, Roy JS, Dionne C, Frémont P, MacDermid JC. The efficacy of therapeutic ultrasound for rotator cuff tendinopathy: A systematic review and meta-analysis. Phys Ther Sport. 2015 Aug;16(3):276-84. doi: 10.1016/j.ptsp.2014.09.004. Epub 2014 Sep 23. PMID: 25824429., https://pubmed.ncbi.nlm.nih.gov/25824429/
(9) Peake JM. Cryotherapy: Are we freezing the benefits of exercise?. Temperature (Austin). 2017;4(3):211-213. Published 2017 Mar 28. doi:10.1080/23328940.2017.1304194, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5605158/
(10) Ohberg L, Lorentzon R, Alfredson H. Eccentric training in patients with chronic Achilles tendinosis: normalised tendon structure and decreased thickness at follow up. Br J Sports Med. 2004 Feb;38(1):8-11; discussion 11. doi: 10.1136/bjsm.2001.000284. PMID: 14751936; PMCID: PMC1724744., https://pubmed.ncbi.nlm.nih.gov/14751936/
(11) 1. Alfredson H, Pietilä T, Jonsson P, Lorentzon R. Heavy-Load Eccentric Calf Muscle Training For the Treatment of Chronic Achilles Tendinosis. The American Journal of Sports Medicine. 1998;26(3):360-366. doi:10.1177/03635465980260030301, ttps://journals.sagepub.com/doi/abs/10.1177/03635465980260030301#articleCitationDownloadContainer
(12) Alfons Mascaró, ,Miquel Àngel Cos, Antoni Morral, Andreu Roig, Craig Purdam, Jill Cook Load management in tendinopathy: Clinical progression for Achilles and patellar tendinopathy Apunts Sports Medicine VOL 53, Issue 197 Pg 19-27 (jan-march 2018)
(13) Abate M, Silbernagel KG, Siljeholm C, et al. Pathogenesis of tendinopathies: inflammation or degeneration?. Arthritis Res Ther. 2009;11(3):235. doi:10.1186/ar2723, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2714139/
(14) Chang, Shu-Wei & Buehler, Markus. (2014). Molecular biomechanics of collagen molecules. Materials Today. 17. 70–76. 10.1016/j.mattod.2014.01.019, https://www.researchgate.net/publication/260914316_Molecular_biomechanics_of_collagen_molecules
(15)Miller BF, Olesen JL, Hansen M, et al. Coordinated collagen and muscle protein synthesis in human patella tendon and quadriceps muscle after exercise. J Physiol. 2005;567(Pt 3):1021-1033. oi:10.1113/jphysiol.2005.093690, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1474228/
(16) Langberg H, Skovgaard D, Petersen LJ, Bulow J, Kjaer M. Type I collagen synthesis and degradation in peritendinous tissue after exercise determined by microdialysis in humans. J Physiol. 1999;521 Pt 1(Pt 1):299-306.
doi:10.1111/j.1469-7793.1999.00299.x, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2269635/
(17) Langberg H, Skovgaard D, Karamouzis M, Bülow J, Kjaer M. Metabolism and inflammatory mediators in the peritendinous space measured by microdialysis during intermittent isometric exercise in humans. J Physiol. 1999;515 ( Pt 3)(Pt 3):919-927. doi:10.1111/j.1469-7793.1999.919ab.x, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2269174/
(18) Buckley MR, Evans EB, Matuszewski PE, et al. Distributions of types I, II and III collagen by region in the human supraspinatus tendon. Connect Tissue Res. 2013;54(6):374-379. doi:10.3109/03008207.2013.847096, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6056177/
(19) Huisman, E., Lu, A., McCormack, R.G. et al. Enhanced collagen type I synthesis by human tenocytes subjected to periodic in vitro mechanical stimulation. BMC Musculoskelet Disord 15, 386 (2014). https://doi.org/10.1186/1471-2474-15-386
(20) Gärdin, A., Movin, T., Svensson, L. et al. The long-term clinical and MRI results following eccentric calf
muscle training in chronic Achilles tendinosis. Skeletal Radiol 39, 435–442 (2010). https://doi.org/10.1007/s00256-009-0798-3
(21) Ackermann, Paul & Franklin, Sarah & Dean, Benjamin & Carr, Andrew & Salo, Paul & Hart, David. (2014). Neuronal pathways in tendon healing and tendinopathy–update. Frontiers in bioscience (Landmark edition). 19. 1251-1278. https://www.researchgate.net/publication/262844530_Neuronal_pathways_in_tendon_healing_and_tendinopathy–update